
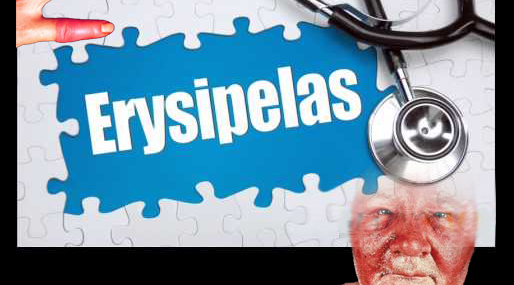
Erysipelas (РОЖА, التهاب الحمرة الجلدي)
Erysipelas (РОЖА, ἐρυσίπελας, Red skin, ignis sacer, holy fire, St. Anthony’s fire, التهاب الحمرة الجلدي) is an acute bacterial dermatological infection caused by b -hemolytic streptococcus group A (bacteria) and involving the upper dermis and subcutaneous tissue that characteristically extends into the regional lymphatic nodes (superficial cutaneous lymphatic nodes, Lymphangitis and lymphadenitis), most commonly, the disease follows a strep throat. Erysipelas is a superficial form of cellulitis.
Classification:
| By the duration of the process | By the nature of local changes |
| 1. Primary erysipelas
2. Recurrent erysipelas 3. Secondary erysipelas |
1. Erythematous form
2. Erythematous -Haemorrhagic form 3. Erythematous-Bullous form 4. Bullus-Hemorrhagic form |
Pathogen: b – hemolytic streptococcus group A
Epidemiology
The source of infection – a patient with streptococcal infection, and Streptococcus carrier.
Mechanism of transmission – aerogenic by ingesting a contaminated airborne droplet, and/or by contact.
Clinical picture
Incubation period of several hours to 5 days, acute start
Intoxication syndrome well expressed with an increase in temperature to reach 40 ° C, severe headache, fatigue, weakness, and nausea.
Focal changes: erythematous, erythematous-hemorrhagic, erythematous-bullous, bullous-hemorrhagic – clearly delineated.
The skin is hot to touch, tense, marked swelling and infiltration, micro hemorrhages in the hemorrhagic components, pustules filled with clear transparent liquid in haemorrhagic and bullous-hemorrhagic components. Regional Lymphangitis and lymphadenitis.
Complications: Abscesses, cellulitis, ulcers, skin necrosis, phlebitis, thrombophlebitis, postulated bullous elements, and secondary elephantiasis (resulting from recurrent erysipelas).
Differential diagnosis
The differential diagnosis is carried out with an abscess, cellulitis, phlebitis, eczema, various types of dermatitis, herpes zoster, pseudoerysipelas, cutaneous anthrax.
Laboratory diagnosis
In blood: moderate leukocytosis with neutrophilic shift to the left, accelerated ESR.
Serological diagnosis: increasing titer of streptococcal antibodies in the PHA.
Treatment
Causal treatment: the drug of choice is penicillin 6 million /day for 7 days, followed by anti-recedive treatment (bitsillin), non-steroidal anti-inflammatory drugs, UFO, UHF on the hearth, aseptic bandage, and detoxification therapy.
Verified by: Dr.Diab (January 7, 2017)
Citation: Dr.Diab. (January 7, 2017). Erysipelas Types Epidemiology Clinic and treatment. Medcoi Journal of Medicine, 6(2). urn:medcoi:article16290.










There are no comments yet
Or use one of these social networks