
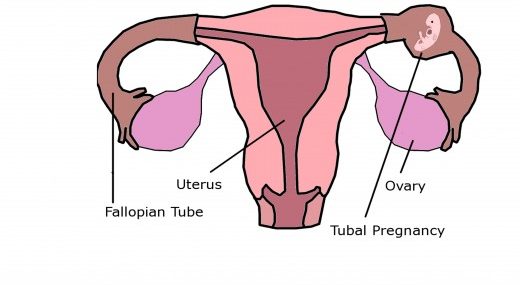
Tubal Pregnancy
What is a tubal pregnancy?
Tubal pregnancy (ectopic pregnancy) is a pathological pregnancy in which implantation occurs outside the uterine cavity in the fallopian tube (oviduct or uterine tube). In most cases, it is caused by a previous tubal infection. Tubal pregnancies usually occur in the ampulla (70.0%), the isthmus (12.0%), the fimbria (11.1%) and the cornua (2.4%).
Tubal pregnancies are the most common type of extrauterine pregnancies or ectopic pregnancies, accounting for 50%-95% of all extrauterine pregnancies. Ectopic pregnancies are pregnancies that occur outside the endometrial cavity in unorthodox locations such as the fallopian tube, cervix, ovary, abdominal or pelvic cavity.
Ovarian, cervical and abdominal pregnancies are extremely rare.
What are the chances of a tubal pregnancy?
Tubal pregnancy affects women of all backgrounds, regardless of race or ethnicity with an incidence rate of one in every 100 pregnancies; However, the incidence of tubal pregnancy is higher in colored women than in white women. The risk of tubal pregnancy increases in women with a tubal disorder, such as PID, previous ectopic pregnancy, etc., women who previously had induced or spontaneous abortions, women who used DES before or during pregnancy, or women who get pregnant while using an IUD (intrauterine device).
How common is an ectopic pregnancy?
Tubal pregnancy occurs in 1% of all pregnancies. In the UK, tubal pregnancies occur in 1%-2% of all pregnancies (around 1 in every 80-90 pregnancies).
It is nearly impossible to get pregnant while using an IUD, since intrauterine devices (IUDs) provide an average efficacy rate of 99.7%.
Pregnancies that persist with an IUD in place are associated with an increased risk of second-trimester miscarriage. If pregnancy occurs with an IUD in place, the IUD should be removed to avoid the risk of second-trimester miscarriage. Second-trimester miscarriage occurs in about half of intrauterine pregnancies if the IUD is not removed within the first 12 weeks of gestation.
An IUD in a pregnant woman increases the risk of second-trimester spontaneous abortion.
Approximately 6% of pregnancies that occur with an IUD in place are ectopic pregnancies.
What are the risks of a tubal pregnancy?
Risk factors for a tubal pregnancy include the following:
- Maternal age of 40-44 years
- Previous tubal pregnancy
- A tubal disorder, such as pelvic inflammatory disease (PID)
- Endometriosis
- Several induced or spontaneous abortions,
- Using DES before or during pregnancy,
- Conceiving while having an IUD in place
- Smoking and obesity
Symptoms
What are the symptoms of a tubal pregnancy?
Early symptoms of a tubal pregnancy usually occur 6 to 8 weeks after a missed period. Common symptoms of tubal pregnancy include:
- Delayed menstruation of more than 3 weeks
- Pale skin
- Low-grade fever
- Abdominal pain that may get worse with movement
- Rebound abdomen, irritation and discomfort when applying pressure just below belly button
- Spotting or abnormal vaginal bleeding, which may be light
What are the side effects of a tubal pregnancy?
Without prompt treatment, the ectopic pregnancy progresses and symptoms get worse over a period of days, or weeks. Symptoms may include:
- Severe abdominal pain that may get worse with movement
- Internal bleeding
- Dyspareunia or painful sexual intercourse
- Heavy vaginal bleeding
- Referred shoulder pain due to diaphragm irritation (Kehr’s sign). Diaphragmatic irritation is caused by internal bleeding into the abdominal cavity (the peritoneal cavity) below the diaphragm. Diaphragmatic irritation often results in pain that radiates to the shoulder
- Dizziness and lightheadedness when standing up
- Syncope or fainting due to internal bleeding (signs of a shock)
If left untreated, the ectopic pregnancy may lead to severe life threatening conditions, such as severe internal bleeding, a worldwide leading cause of maternal mortality.
How long does it take for an ectopic pregnancy to rupture?
An ectopic pregnancy is likely to rupture the wall of the fallopian tube roughly 6 to 8 weeks after conception, long before the fetus is viable. However, an ectopic pregnancy that implants partly in the uterus and partly in the fallopian tube usually ruptures 12 to 16 weeks after conception.
When a tubal pregnancy ruptures, bleeding may be severe and can lead to death if not treated promptly.
Causes
What causes a tubal pregnancy?
In most cases a tubal implantation is believed to be caused by a previous tubal infection, it is the most common type of ectopic pregnancies where implantation occurs outside of the uterine cavity (the endometrium or endometrial cavity), known sites are the uterine tube, ovaries, abdominal or pelvic cavity.
In most cases, tubal pregnancies are caused by one or more of the following:
Fallopian tube blockage due to salpingitis, an inflammation of the fallopian tube caused by bacterial infection. Endometriosis can cause irritation, or inflammation of the fallopian tube and in severe cases, it can lead to fallopian tube blockage due to the formation of scar tissue or adhesions.
Complications after fallopian tube surgery, when scar tissue forms at the very end of the fallopian tubes. It is the most common cause of tubal blockage
Scar tissue and adhesions from a previous pelvic inflammatory infection may also impede the egg’s movement.
Adhesions due to a previous fallopian tube surgery or surgery in the pelvic area.
Congenital fallopian tube disorders can result in an abnormality in the tube’s shape.
Next steps management
How to diagnose a tubal pregnancy?
In the reanimation:
- Infusion therapy
- Transvaginal ultrasound is the gold standard for diagnosis of ectopic pregnancy. A transvaginal ultrasound showing no gestational sac in the uterus with a high hCG level (above 1,500) confirms a diagnosis of ectopic pregnancy. Ectopic pregnancies can also be detected using a pelvic exam.
- Diagnostic tests for hemoglobin, leukocytes and blood group
- Testing hCG levels, hCG can be detected in a blood test 11 days after conception; However, hCG continue to double every 48 to 72 hours until they reach their peak around 8-11 weeks after conception. After that, hCG levels start to decline.
- Surgical treatment
Treatment
How to treat a tubal pregnancy?
The main treatment options are:
Expectant management and careful medical monitoring by a physician for a 14-day period, during this period pain or bleeding should lessen or stop completely. However, if you haven’t had any pain or bleeding within 7-14 days, or if the symptoms get worse after 7-10 days, this could mean that the abortion hasn’t begun or hasn’t completely finished.
Methotrexate (MTX or amethopterin) is a chemotherapy drug and immunosuppressant commonly used to stop the embryonic cells from growing (dividing and multiplying). Patients with a diagnosis of tubal pregnancy are given 2.5 mg of methotrexate for 5 days orally or a single dose of methotrexate, 75 mg intramuscularly (75-50 mg/m2) and 25-50 mg orally followed by 800 micrograms misoprostol vaginally. Misoprostol should be given 5-6 days after initiation of treatment with methotrexate. The misoprostol dose should be repeated if the abortion is not complete.
Patients should receive a test dose of 2.5 mg of Methotrexate to exclude unexpected and toxic effects.
Laparoscopy is a surgical procedure used to remove the embryo along with the affected fallopian tube (laparoscopic removal of the embryo from the lumen). Alternatively, a tubal pregnancy can be removed from a fallopian tube by using laparoscopic salpingectomy or laparoscopic tubectomy (fimbriectomy) and resection (removal) of a portion of the fallopian tube.
Methotrexate can also be used after surgical treatment to ensure that all embryonic cell growth has stopped.
Prognosis
Can a baby survive in an ectopic pregnancy?
Sadly, during a tubal pregnancy, the fetus can never be born alive.
Tubal pregnancy is a leading cause of maternal morbidity and mortality, severe internal bleeding can cause life threatening conditions and, can lead to a maternal death secondary to ruptured ectopic pregnancy.
Ruptured tubal pregnancy accounts for 10% to 15% of maternal mortality worldwide. In 2015, the global maternal mortality ratio was estimated at 216 deaths per 100,000 live births.
Verified by: Dr.Diab (November 20, 2017)
Citation: Dr.Diab. (November 20, 2017). What is a Tubal Pregnancy? Causes Symptoms and Treatment. Medcoi Journal of Medicine, 15(2). urn:medcoi:article15611.










There are no comments yet
Or use one of these social networks